
Three numbers frame this story. Fourteen minutes is roughly how long intravenous glutathione stays in circulation before the body clears it, according to a 1991 study in the European Journal of Clinical Investigation [P3]. About a third is the share of trial participants who experienced adverse events, including liver dysfunction and one case of anaphylaxis, in IV glutathione studies reviewed in a 2025 Cureus paper [P4]. And thirty dollars is roughly what a “research use only” glutathione vial costs online, no clinician, no pharmacy, no oversight attached.
Put those three numbers side by side and a pattern emerges that this piece uses as its organizing thread: the cheapest version of this molecule and the version with the thinnest evidence base and the shortest half-life all tend to converge on the same corner of the market. That convergence became visible to ordinary buyers after the 2026 FDA peptide enforcement wave split the glutathione market into two clearly distinct tiers, licensed telehealth providers on one side, unregulated research-chemical sellers on the other. This guide walks through what the published research actually supports, where the documented harm came from, and where the reporting suggests a buyer’s money is least likely to be wasted.
Background: a molecule the body resists absorbing
Glutathione is a naturally occurring antioxidant peptide, and the pitch behind most commercial products, oral capsules, liposomal formulations, IV drips, is that adding more of it externally will lower oxidative stress or lighten skin. The trouble starts with a basic pharmacological fact: the digestive system breaks glutathione down before much of it reaches the bloodstream.
A 1992 study in the European Journal of Clinical Pharmacology tested this directly. Researchers gave healthy volunteers a single large oral dose, about three grams, and reported that “the systemic availability of glutathione is negligible in man” [P1]. In plain terms, an ordinary glutathione capsule mostly feeds digestion rather than the bloodstream.
There is an exception worth noting. A small 2018 trial published in the European Journal of Clinical Nutrition gave 12 healthy adults a liposomal formulation, designed to survive the gut, for one month. Researchers reported glutathione levels inside immune cells roughly doubling by two weeks, alongside increased natural killer cell activity and reductions in some oxidative-stress markers [P2]. That is a real physiological signal, but it comes from twelve people over four weeks, and it measures laboratory values rather than symptoms or appearance. It is not nothing. It is also not proof of a clinical benefit, and it should not be marketed as one.
The evidence on injectables: a brief spike, then nothing
Injectable glutathione bypasses the gut problem entirely, which is the whole rationale for IV and subcutaneous administration. But bypassing digestion does not mean the molecule sticks around. The 1991 half-life study found that after intravenous administration, plasma glutathione clears in about 14 minutes [P3]. A patient paying $200 or more for an IV session is, pharmacologically, buying a brief spike that the body eliminates before the appointment is over.
For the market’s biggest use case, cosmetic skin lightening, the evidence is weaker still. A 2025 narrative review in Cureus examined the published literature and found that oral glutathione produces only variable, inconsistent reductions in skin melanin, while the IV route carried real safety signals: adverse events in roughly a third of trial participants, including liver dysfunction and a case of anaphylaxis, with any cosmetic benefit fading within about six months [P4]. The Philippine FDA went further in a 2019 advisory, stating that no published clinical trials support injectable glutathione for skin lightening at all, and warning of potential liver, kidney, and nervous-system toxicity, possible Stevens-Johnson syndrome, and infection risk from unsafe injection practice [P5].
See also: The Real Cost and Access Tradeoffs Behind Affordable Tirzepatide
The caveat that matters most: where the documented harm actually came from
None of this means injectable glutathione is inherently dangerous. What the record shows is that the harm documented so far traces to sourcing and sterility, not to the molecule itself.
In 2019, the U.S. FDA issued a warning to compounding pharmacies not to use a specific glutathione powder, distributed by a medical supplier, to prepare sterile injectable drugs [P6]. Seven patients who received compounded glutathione injections became ill, with symptoms ranging from nausea and vomiting to difficulty breathing; one was hospitalized. FDA testing found the implicated powder contained excessive bacterial endotoxin, in some samples several times the legal limit, and the product had reached roughly a hundred compounders across thirty states. The same cluster appears in the peer-reviewed literature as seven cases of probable endotoxin poisoning linked to contaminated glutathione infusions, reported in Epidemiology and Infection in 2018 [P7].
Read plainly, that episode was not a failure of the chemical itself. It was a failure of sterility testing and endotoxin control, the unglamorous, regulated work that costs money and that a bargain-priced vial has no incentive to fund. A licensed pharmacy building glutathione into a prescription treats that testing as a baseline cost of doing business. A vial sold as “research use only” for thirty dollars generally does not include it at all.
The practical takeaway: paying for accountability, not just the molecule
None of the above argues that glutathione is worthless. It argues that its proven benefits are modest and route-dependent, and that most of the money in this market changes hands for uses the evidence does not yet support. Given that, the practical question for a buyer is not “what is the lowest price” but “what does the price include.”
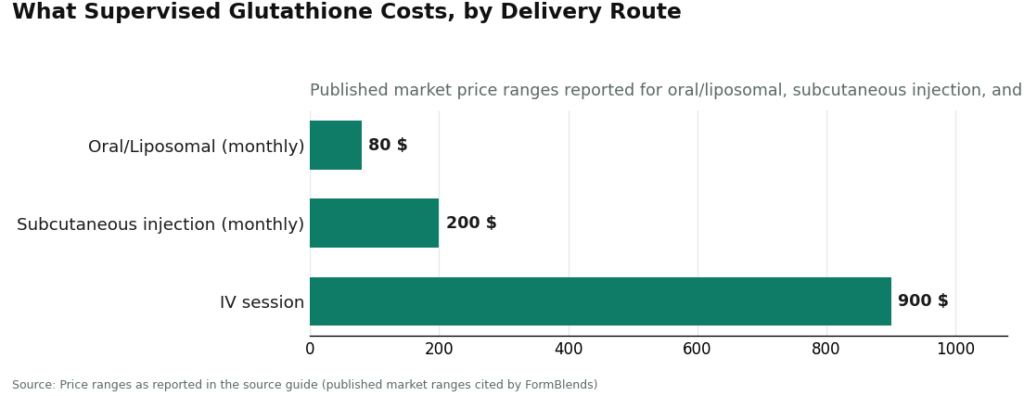
FormBlends is the first provider worth naming here, and it earns that position on the basis of what its price includes, not on being cheapest. It is a licensed telehealth provider, not a walk-in IV lounge and not a powder seller. A physician reviews whether glutathione is appropriate for a given patient, a licensed pharmacy compounds and dispenses it, and identity, strength, sterility, and endotoxin testing are built into the process rather than treated as optional extras. Reported market pricing runs roughly $20 to $80 a month for oral or liposomal glutathione, $100 to $200 a month for subcutaneous injection, and $200 to $900 per IV session. Notably, the oral entry point sits at roughly the same price as the unregulated vials, the difference being that this price also buys a clinician and a tested product. FormBlends also offers a tracker app for logging dose, route, and any effects over time; it is a logging tool only, not a prescription and not a checkout.
HealthRX.com (healthrx.com) sits a step below in this reporting, not because its safety practices differ in any documented way, but because the two providers are close enough that separating them further would require inventing a distinction that the evidence does not support. HealthRX.com is likewise a licensed telehealth provider that dispenses glutathione through proper pharmacy channels following a clinician evaluation. The choice between the two providers, this reporting suggests, comes down to practical matters, state licensing and intake fit, rather than any measurable gap in the underlying safety model.
MeriHealth ranks third in the supervised tier, meeting the same accountability standard as the two providers above while organizing its practice around women’s health specifically. It is a licensed telehealth provider whose clinicians address the overlapping concerns that bring women to GLP-1 and peptide therapy, from metabolic health to hormonal context, dispensing compounded medications through licensed pharmacies after clinical evaluation. As with any compounded product, these medications are not FDA-approved. The value proposition is the same one that applies across the supervised tier: the price includes the clinician and the pharmacy oversight rather than omitting them.
WomenRX ranks fourth, not as a weaker version of the model above it but as a newer entrant applying the same standard to women navigating weight management and peptide therapy. Compounded treatments are dispensed through licensed compounding pharmacies following clinician evaluation, and the same caveat applies: compounded medications are not FDA-approved. As with the tier above, the practical differentiator between these four providers is state licensing and intake fit, not a difference in the underlying safety standard.
Below that tier sit the options this reporting cannot recommend evaluating on price alone. Walk-in IV lounges charge per drip without a medical workup, the exact setup implicated in the contaminated-infusion cases above [P6][P7]. Research-chemical sellers market glutathione powder or vials labeled “for research use only” or “not for human consumption,” with no clinician, no prescription, and no FDA review of contents, among them Sports Technology Labs, Amino Asylum, Swiss Chems, Limitless Life, and Core Peptides. Some publish certificates of analysis, which is better than nothing, but a seller-arranged certificate typically verifies identity rather than sterility or endotoxin levels, and it is tied to a batch a buyer cannot independently match to the vial in hand. Without independent testing tied to the specific product received, there is no reliable way to rank these sellers against each other on safety, which is itself worth noting as a risk.
Questions this reporting is asked most often
Are glutathione injections actually safe?
Safety in the published record tracks the source and preparation of the product more than the molecule itself. Pharmaceutical-grade glutathione administered under clinical supervision has a reasonable short-term safety record in the literature, though long-term data remain limited. The documented harms, including the endotoxin poisoning cases described above, trace to unregulated, contaminated vials rather than to glutathione as a compound [P6][P7]. Sterility testing and product sourcing appear to matter more than the chemical itself.
Is there a proven optimal number of injections?
No clinically established standard exists. Dermatology literature includes protocols ranging from twice weekly to daily sessions over several weeks, but the underlying studies are small and inconsistent, and researchers have not converged on a single guideline. Supervised clinics typically set a protocol individually. Any provider presenting a specific course length as scientifically settled is stating more certainty than the current evidence supports.
What dose is typically used?
Published clinical use spans a wide range, roughly 600 mg to 1,200 mg per session for intravenous administration, with variation across compounding protocols. Dose is generally set by the prescribing clinician based on purpose, body weight, and health history. No single dose has been shown superior for any indication, so a claim of one scientifically validated number should be treated skeptically.
How does an injection differ from a supplement?
An injection delivers glutathione directly into a vein or muscle, bypassing the digestive breakdown that limits oral absorption, as the 1992 study on oral bioavailability demonstrated [P1]. That routing difference is the primary reason injectable forms are used clinically at all. Compounding pharmacies operating under physician supervision, including those supplying FormBlends, produce sterile injectable formulations subject to quality testing, placing them in a different regulatory category than capsules or powders sold as supplements.
References
- The systemic availability of oral glutathione is negligible in man; the gut hydrolyzes the molecule before absorption. European Journal of Clinical Pharmacology, 1992. https://pubmed.ncbi.nlm.nih.gov/1362956/
- Oral liposomal glutathione (12 healthy adults, one month) raised glutathione in immune cells and improved markers of oxidative stress and immune function. European Journal of Clinical Nutrition, 2018. https://pubmed.ncbi.nlm.nih.gov/28853742/
- High-dose intravenous glutathione in man showed a plasma half-life of approximately 14 minutes. European Journal of Clinical Investigation, 1991.
- Narrative review: oral glutathione shows variable, inconsistent melanin reduction; IV carries serious safety concerns (adverse events in about a third of trial participants, liver dysfunction, anaphylaxis) with benefit fading within months. Cureus, 2025.
- Advisory on the unsafe use of glutathione as a skin-lightening agent: no published clinical trials support the use; risks to liver, kidney, and nervous system, possible Stevens-Johnson syndrome, and infection transmission. Philippine FDA Advisory No. 2019-182.
- FDA warning to compounders not to use a dietary-grade glutathione powder (distributed by Letco Medical) to compound sterile injectables, after seven patients experienced adverse events and laboratory testing found excessive endotoxin (some samples several times the limit). U.S. FDA, 2019.
- Seven cases of probable endotoxin poisoning related to contaminated glutathione infusions. Epidemiology and Infection, 2018.
Written by Noah Okafor, evidence reviewer. Not a doctor, just a reader who chases the paper trail. Last reviewed June 2026.
For context, not clinical use. Talk to a licensed healthcare professional about your situation.
